
Click here to see all images
April, 2026
Case of the Month
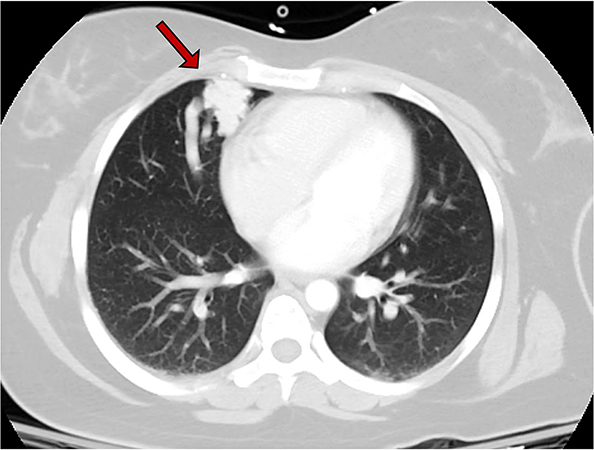
Clinical History: A 30-year-old woman underwent a chest computed tomography (CT) scan after a motor vehicle accident which showed an incidental 2.6 cm pulmonary ‘vascular’ lesion in the anteromedial right middle lobe (Figure 1, arrow). The patient reported symptoms of post-exertional dyspnea, intermittent mid-sternal pain, and easy bleeding. Physical exam showed clubbing of fingers but no other relevant findings. Pulmonary function tests showed a FEV1 of 2.58 (82% predicted), and DLCO of 14.17 (65% predicted). Her cardiovascular reserve was preserved with 88% SpO2 at 4 minutes in a 6-minute walk test. CT angiogram demonstrated many feeding arteries to the pulmonary lesion to allow for embolization. Subsequently, the patient underwent right middle lobectomy. Grossly, the lesion was composed of numerous vascular spaces and was relatively well-circumscribed from the adjacent lung (Figure 2). A full montage scan (Figure 3) and representative photomicrographs of the lesion at 4X magnification are shown (Figure 4, H&E; Figure 5, trichrome).Q1. What is the diagnosis?
- Pulmonary hemangioma
- Pulmonary lymphangioma
- Pulmonary artery pseudoaneurysm
- Pulmonary arteriovenous malformation
Q2. Which genetic disorder can be associated with multiple of these lung lesions
- Birt-Hogg-Dubé syndrome
- Osler-Weber-Rendu syndrome
- von Recklinghausen syndrome
- Sturge-Weber syndrome
Q3. What features best describe the histopathology of this lesion?
- Thick-walled vessels with variable amounts of elastic fibers, smooth muscle and collagen
- Thin-walled vascular spaces lined by endothelial cells: D2-40+, CD31+, CD34-/+
- Pulmonary artery with disrupted medial wall with decrease in elastic fibers
- Vascular proliferation with ectatic channels lined by endothelium and complete smooth muscle wall
Answers to Quiz
Q1. D
Q2. B
Q3. A
Q2. B
Q3. A
Diagnosis
Pulmonary arteriovenous malformation (PAVM)
Discussion
Pulmonary arteriovenous malformations (PAVMs) are rare and occur two times more frequently in females than males. They originate from persistent anastomotic fetal capillaries and may be asymptomatic or symptomatic. The latter are characterized by a pathological right-to-left shunt that disrupts normal gas exchange and venous blood filtration in the pulmonary circulation.
PAVMs can be divided into congenital and sporadic. Most cases are congenital and occur in patients with hereditary hemorrhagic telangiectasia (HHT), also known as Osler-Weber-Rendu syndrome (autosomal dominant). The other syndromes listed above are associated with vascular lesions at other sites, but not with PAVM. One-third of patients with more than one PAVM have HHT, but this association may also occur with isolated lesions. Therefore, thorough clinical evaluation and genetic testing is important to exclude HHT. The patient from this case had a history of easy bleeding but no telangiectasias and her genetic testing for HHT was negative. Genetic mutations in HHT and PAVMs include those affecting proteins involved in vascular development, such as ENG (endoglin, CD105), ACVRL1 (activin receptor-like-kinase-1), and SMAD4, all playing a specific function in the TGF-β (transforming growth factor-β) signaling pathway. This pathway has crucial effects in angiogenesis and vascular homeostasis. Congenital PAVM may also occur in patients with dyskeratosis congenita, a short-telomere disorder. Sporadic PAVMs have multiple etiologies, developing secondary to infections, prior surgery, trauma, certain heart conditions, and lung metastasis.
Nowadays, surgical intervention is rarely performed as definitive treatment for PAVM, with most cases diagnosed via imaging (Figure 1) and resolved by therapeutic embolization. For this reason, gross specimens of PAVM are infrequent (Figure 2). Grossly, they range from numerous dilated vascular spaces to single large structures, sometimes dilated and mimicking an aneurysm. Microscopically, PAVM is composed of variable number of thick-walled vessels of different sizes with variable amounts of elastic fibers, smooth muscle and collagen (Figures 3-5). PAVMs with dilated vessels may resemble aneurysms and those with thin-walled vessels may mimic hemangiomas, but they tend to show more classic features in other areas. A disrupted medial wall with decrease in elastic fibers is a feature of an aneurysm and not PAVM, while thin-walled vessels are typical of hemangioma. Vascular lesions with thin-walled vascular spaces lined by D2-40+, CD31+, CD34-/+ endothelial cells are lymphangiomas.
Take home message for trainees:
PAVM is a rare vascular lesion that may be asymptomatic or symptomatic, with a pathological right-to-left shunt that disrupts normal gas exchange and the pulmonary circulation. Most cases are congenital and occur in patients with hereditary hemorrhagic telangiectasia. Although most patients with HHT present with multiple PAVMs, an isolated lesion still requires thorough clinical and genetic evaluation given the clinical implications. Microscopically, PAVM is characterized by thick-walled vessels with variable amounts of elastic fibers, smooth muscle and collagen. Most of these lesions are rarely resected since they are typically resolved by therapeutic embolization.
PAVMs can be divided into congenital and sporadic. Most cases are congenital and occur in patients with hereditary hemorrhagic telangiectasia (HHT), also known as Osler-Weber-Rendu syndrome (autosomal dominant). The other syndromes listed above are associated with vascular lesions at other sites, but not with PAVM. One-third of patients with more than one PAVM have HHT, but this association may also occur with isolated lesions. Therefore, thorough clinical evaluation and genetic testing is important to exclude HHT. The patient from this case had a history of easy bleeding but no telangiectasias and her genetic testing for HHT was negative. Genetic mutations in HHT and PAVMs include those affecting proteins involved in vascular development, such as ENG (endoglin, CD105), ACVRL1 (activin receptor-like-kinase-1), and SMAD4, all playing a specific function in the TGF-β (transforming growth factor-β) signaling pathway. This pathway has crucial effects in angiogenesis and vascular homeostasis. Congenital PAVM may also occur in patients with dyskeratosis congenita, a short-telomere disorder. Sporadic PAVMs have multiple etiologies, developing secondary to infections, prior surgery, trauma, certain heart conditions, and lung metastasis.
Nowadays, surgical intervention is rarely performed as definitive treatment for PAVM, with most cases diagnosed via imaging (Figure 1) and resolved by therapeutic embolization. For this reason, gross specimens of PAVM are infrequent (Figure 2). Grossly, they range from numerous dilated vascular spaces to single large structures, sometimes dilated and mimicking an aneurysm. Microscopically, PAVM is composed of variable number of thick-walled vessels of different sizes with variable amounts of elastic fibers, smooth muscle and collagen (Figures 3-5). PAVMs with dilated vessels may resemble aneurysms and those with thin-walled vessels may mimic hemangiomas, but they tend to show more classic features in other areas. A disrupted medial wall with decrease in elastic fibers is a feature of an aneurysm and not PAVM, while thin-walled vessels are typical of hemangioma. Vascular lesions with thin-walled vascular spaces lined by D2-40+, CD31+, CD34-/+ endothelial cells are lymphangiomas.
Take home message for trainees:
PAVM is a rare vascular lesion that may be asymptomatic or symptomatic, with a pathological right-to-left shunt that disrupts normal gas exchange and the pulmonary circulation. Most cases are congenital and occur in patients with hereditary hemorrhagic telangiectasia. Although most patients with HHT present with multiple PAVMs, an isolated lesion still requires thorough clinical and genetic evaluation given the clinical implications. Microscopically, PAVM is characterized by thick-walled vessels with variable amounts of elastic fibers, smooth muscle and collagen. Most of these lesions are rarely resected since they are typically resolved by therapeutic embolization.
References
Danyalian A, Sankari A, Hernandez F. Pulmonary arteriovenous malformation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Bookshelf ID: NBK560696.
Meier NM, Foster ML, Battaile JT. Hereditary hemorrhagic telangiectasia and pulmonary arteriovenous malformations: clinical aspects. Cardiovasc Diagn Ther. 2018;8:316-24. PMID: 30057878
Cullivan S, Kevane B, McCullagh B, O'Connor TM, Condliffe R, Gaine S. Pulmonary vascular manifestations of hereditary haemorrhagic telangiectasia. Pulm Circ. 2024;14:e70007. PMID: 39588537
Fraire AE, Dail DH. Chapter 40: Mesenchymal tumors, part II: Tumors of hamartomatous, osteochondromatous, lipomatous, neural and vascular origin. In: Dail and Hammar’s Pulmonary Pathology. Tomashefski JF, Cagle PT, Farver CF, Fraire AE (eds) 3rd ed. Volume I: Neoplastic lung disease. 2008. pp. 476-7.
Meier NM, Foster ML, Battaile JT. Hereditary hemorrhagic telangiectasia and pulmonary arteriovenous malformations: clinical aspects. Cardiovasc Diagn Ther. 2018;8:316-24. PMID: 30057878
Cullivan S, Kevane B, McCullagh B, O'Connor TM, Condliffe R, Gaine S. Pulmonary vascular manifestations of hereditary haemorrhagic telangiectasia. Pulm Circ. 2024;14:e70007. PMID: 39588537
Fraire AE, Dail DH. Chapter 40: Mesenchymal tumors, part II: Tumors of hamartomatous, osteochondromatous, lipomatous, neural and vascular origin. In: Dail and Hammar’s Pulmonary Pathology. Tomashefski JF, Cagle PT, Farver CF, Fraire AE (eds) 3rd ed. Volume I: Neoplastic lung disease. 2008. pp. 476-7.
Contributors
Sergio Pina-Oviedo, MD
Associate Professor
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Haijun “Steve” Zhou, MD, PhD
Associate Professor and Associate Director of Pulmonary Pathology
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Seema S. Mullick, MD
Associate Professor
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Roberto Barrios, MD
Professor and Director of Pulmonary Pathology
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Associate Professor
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Haijun “Steve” Zhou, MD, PhD
Associate Professor and Associate Director of Pulmonary Pathology
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Seema S. Mullick, MD
Associate Professor
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX
Roberto Barrios, MD
Professor and Director of Pulmonary Pathology
Department of Pathology & Genomic Medicine
Houston Methodist Hospital
Houston, TX