
Click here to see all images
February, 2026
Case of the Month
Clinical History:A 31-year-old man, who underwent a double lung transplant for cystic fibrosis in 2008 and a deceased donor kidney transplant in 2017, was admitted in June 2025 for evaluation of bilateral cavitated lung lesions. He is currently asymptomatic, denying fever, dyspnea, cough, sputum production, chest pain, or other symptoms. He is a non-smoker and does not consume alcohol or other drugs. He reports that in early May 2025, he experienced a cough with brownish sputum, for which his physician prescribed cefuroxime and fluidasa, resulting in clinical improvement. Currently, he presents a non-productive cough without other symptoms.
The chest CT scan from July 3, 2025, shows cavitated consolidations: one in the right upper lobe (RUL) measuring 3 cm and another in the right lower lobe (RLL) of 2.5 cm, along with small non-cavitated consolidation foci predominantly in the right hemithorax. A partially loculated right pleural effusion and a small left pleural effusion are also present. Given the negative culture results, clinical stability, and the need to rule out neoplasia, a surgical biopsy was performed, and a sample was sent for intraoperative study.
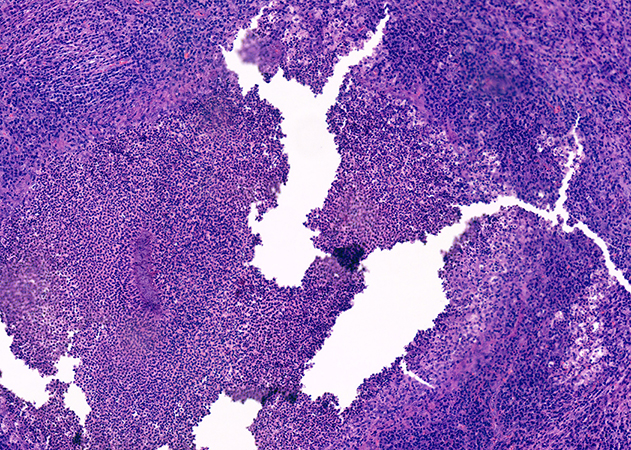
The submitted material consisted of fragments of lung parenchyma with firm consistency and poorly defined whitish-yellow areas. No evident tumor masses were identified. The intraoperative study (Figure 1) showed chronic suppurative inflammation with abundant infiltrate of neutrophils, lymphocytes, and plasma cells, associated with areas of necrosis and microabscesses. In the subsequent deferred study, rounded basophilic granules were identified, consisting of bacterial colonies with a central filamentous arrangement and a peripheral eosinophilic halo (Splendore-Hoeppli phenomenon) (Figures 2 and 3). Gram staining revealed Gram-positive filamentous bacilli (Figure 4). Grocott staining was positive (Figure 5), highlighting filamentous structures. Ziehl-Neelsen staining was negative (Figure 6).
Q1. What diagnoses are suggested by the intraoperative biopsy?
- Metastatic neoplasia
- Necrotizing granulomas
- Non-neoplastic and microabscesses
- Lymphoproliferative process in a transplant patient
Q2. What differential diagnoses do you consider based on the stain results?
- Tuberculosis
- Lymphoproliferative process in a transplant patient
- Aspiration pneumonia
- Actinomyces, Nocardia, Aspergillus
Q3. What medical consultation would you suggest the clinicians perform?
- Oncology Department
- Preventive Medicine Department
- Maxillofacial Surgery Department
- Hematology Department
Answers to Quiz
Q1. C
Q2. D
Q3. C
Q2. D
Q3. C
Diagnosis
Lung with chronic suppurative granulomatous inflammation associated with bacterial colonies compatible with pulmonary actinomycosis.
Discussion
Pulmonary actinomycosis is an infection caused by anaerobic filamentous bacteria within the Actinomycetales family. It is usually the result of aspiration of infected material or extension of a cervicofacial infection and can be mistaken for a neoplastic process. In our case, once the biopsy was reported, the oral cavity was examined, revealing deteriorated right lower teeth with cavities in tooth 36 and a significant cavity with an apical lesion in tooth 34. The Maxillofacial Surgery Department identified this as the possible source of the current process. Extraction of tooth 34 and curettage were performed. Currently, the patient is asymptomatic and continues the prescribed antibiotic treatment for one year.
Take home message for trainees: In an immunocompromised patient with these findings, it is essential to primarily rule out neoplastic processes, tuberculosis, Nocardia, fungal infections such as aspergillosis and mucormycosis, and chronic bacterial lung abscess. The identification of sulfur granules (which Nocardia does not present) together with filamentous Gram-positive bacilli that are not acid-fast and are Grocott-positive allows for the diagnosis of pulmonary actinomycosis.
Take home message for trainees: In an immunocompromised patient with these findings, it is essential to primarily rule out neoplastic processes, tuberculosis, Nocardia, fungal infections such as aspergillosis and mucormycosis, and chronic bacterial lung abscess. The identification of sulfur granules (which Nocardia does not present) together with filamentous Gram-positive bacilli that are not acid-fast and are Grocott-positive allows for the diagnosis of pulmonary actinomycosis.
References
Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183-197. doi:10.2147/IDR.S39601. PMID: 25045274.
Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003;21(3):545-551. doi:10.1183/09031936.03.00089103. PMID: 12662015.
Bassiri AG, Girgis RE, Theodore J. Actinomyces odontolyticus thoracopulmonary infections. Two cases in lung and heart-lung transplant recipients and a review of the literature. Chest. 1996;109(4):1109-1111. doi:10.1378/chest.109.4.1109. PMID: 8635341.doi:10.1016/j.chest.2024.06.770.
Fayos M, Severo A, García-Cosío MD, Prados C, Alonso M, López-Medrano F. Nocardia and mucoral co-infection in heart transplant recipient. Rev Esp Quimioter. 2024;37(6):523-526. doi:10.37201/req/075.2024. PMID: 39387191.
Martínez-Girón R, Pantanowitz L. Pulmonary actinomycosis: cytomorphological features. Monaldi Arch Chest Dis. 2021;92(2):1641. doi:10.4081/monaldi.2021.1641. PMID: 34738778.
Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003;21(3):545-551. doi:10.1183/09031936.03.00089103. PMID: 12662015.
Bassiri AG, Girgis RE, Theodore J. Actinomyces odontolyticus thoracopulmonary infections. Two cases in lung and heart-lung transplant recipients and a review of the literature. Chest. 1996;109(4):1109-1111. doi:10.1378/chest.109.4.1109. PMID: 8635341.doi:10.1016/j.chest.2024.06.770.
Fayos M, Severo A, García-Cosío MD, Prados C, Alonso M, López-Medrano F. Nocardia and mucoral co-infection in heart transplant recipient. Rev Esp Quimioter. 2024;37(6):523-526. doi:10.37201/req/075.2024. PMID: 39387191.
Martínez-Girón R, Pantanowitz L. Pulmonary actinomycosis: cytomorphological features. Monaldi Arch Chest Dis. 2021;92(2):1641. doi:10.4081/monaldi.2021.1641. PMID: 34738778.
Contributors
Angeles Gómez López
Laboratory Technician
Department of Pathology, CHUAC, Spain.
Antía Rodríguez López
Resident Physician
Department of Pathology, CHUAC, Spain.
Teresa Hermida Romero, MD
Thoracic Pathology
Department of Pathology, CHUAC, Spain.
Laboratory Technician
Department of Pathology, CHUAC, Spain.
Antía Rodríguez López
Resident Physician
Department of Pathology, CHUAC, Spain.
Teresa Hermida Romero, MD
Thoracic Pathology
Department of Pathology, CHUAC, Spain.