2026 PPS Lifetime Achievement Award
William D. Travis, MD
2026 PPS Biennial Meeting Handouts (requires membership login)
2026 PPS Biennial Videos.
The PPS Biennial videos are now available to registrants of the meeting. If you didnot register and attend the live meeting, you may purchase accesss to the videos for a reduced price at the virtual registration page. Note that this purchase provides access to
the videos, but does not include CME.
April Case of the Month Clinical History:
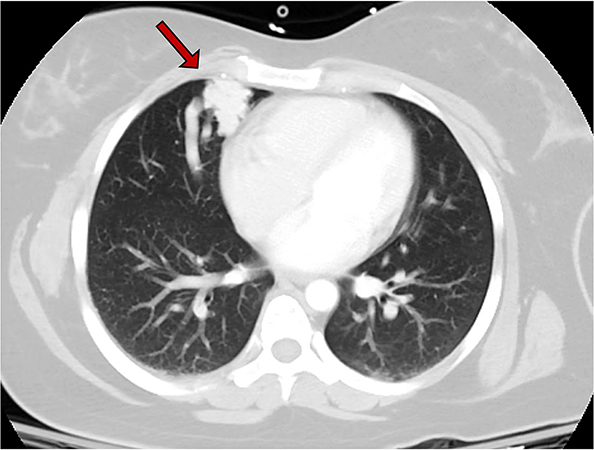
A 30-year-old woman underwent a chest computed tomography (CT) scan after a motor vehicle accident which showed an incidental 2.6 cm pulmonary ‘vascular’ lesion in the anteromedial right middle lobe (Figure 1, arrow). The patient reported symptoms of post-exertional dyspnea, intermittent mid-sternal pain, and easy bleeding. Physical exam showed clubbing of fingers but no other relevant findings. Pulmonary function tests showed a FEV1 of 2.58 (82% predicted), and DLCO of 14.17 (65% predicted). Her cardiovascular reserve was preserved with 88% SpO2 at 4 minutes in a 6-minute walk test. CT angiogram demonstrated many feeding arteries to the pulmonary lesion to allow for embolization. Subsequently, the patient underwent right middle lobectomy. Grossly, the lesion was composed of numerous vascular spaces and was relatively well-circumscribed from the adjacent lung (Figure 2). A full montage scan (Figure 3) and representative photomicrographs of the lesion at 4X magnification are shown (Figure 4, H&E; Figure 5, trichrome)..
Click here to see more.
A 30-year-old woman underwent a chest computed tomography (CT) scan after a motor vehicle accident which showed an incidental 2.6 cm pulmonary ‘vascular’ lesion in the anteromedial right middle lobe (Figure 1, arrow). The patient reported symptoms of post-exertional dyspnea, intermittent mid-sternal pain, and easy bleeding. Physical exam showed clubbing of fingers but no other relevant findings. Pulmonary function tests showed a FEV1 of 2.58 (82% predicted), and DLCO of 14.17 (65% predicted). Her cardiovascular reserve was preserved with 88% SpO2 at 4 minutes in a 6-minute walk test. CT angiogram demonstrated many feeding arteries to the pulmonary lesion to allow for embolization. Subsequently, the patient underwent right middle lobectomy. Grossly, the lesion was composed of numerous vascular spaces and was relatively well-circumscribed from the adjacent lung (Figure 2). A full montage scan (Figure 3) and representative photomicrographs of the lesion at 4X magnification are shown (Figure 4, H&E; Figure 5, trichrome)..
Click here to see more.